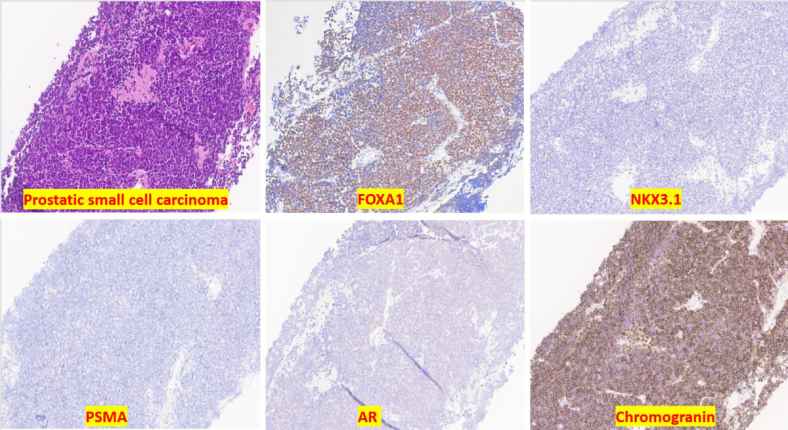
A diagnostic marker called FOXA1 could help diagnose aggressive forms of prostate cancer that often go undetected due to lost traditional markers. Researchers at MD Anderson Cancer Center found that FOXA1 expression is notably higher in prostate cancer and similar to another marker, NKX3.1.
The detectable expression of the FOXA1 protein makes it a potentially viable option for diagnosing aggressive subtypes of prostate cancer that often lose conventional markers such as NKX3.1, according to researchers at The University of Texas MD Anderson Cancer Center. This study was published in Histopathology and led by Jianping Zhao, M.D., Ph.D., assistant professor of Anatomic Pathology.
According to Dr. Zhao, "The detectable expression of FOXA1 in most small cell carcinomas of the prostate makes it a potentially viable option for diagnosing aggressive subtypes that lose conventional markers." While further study is needed to understand the specific molecular mechanisms behind this marker's effectiveness, these results are encouraging as they could help pathologists make more accurate prognostic and therapeutic decisions.
Prostate cancer treatment often includes androgen deprivation therapy. However, some aggressive forms of prostate cancer develop resistance independently from androgens, leading to a poorer prognosis for patients. Small cell carcinoma of the prostate is one such common and aggressive form that can be difficult to diagnose because it frequently loses expression of standard markers like NKX3.1.
This loss in traditional markers makes it challenging to determine whether metastatic tumors are the result of progression from known tumors within the prostate or new primary tumors originating elsewhere. The researchers at MD Anderson Cancer Center used data from The Cancer Genome Atlas database and found FOXA1 as a potential candidate for diagnosing these aggressive subtypes.
To study FOXA1 expression, the team analyzed tissue samples from both primary and metastatic prostate tumors as well as other cancer types. They discovered that FOXA1 expression was notably higher in prostate cancer cases and showed similar levels to NKX3.1. Interestingly, they detected FOXA1 expression in 80% of primary and 57% of metastatic small cell carcinomas of the prostate, indicating its potential value as a diagnostic tool.
Further evaluation is needed to understand FOXA1's role in other aggressive subtypes of prostate cancer and to comprehend its molecular mechanisms. Prospective clinical studies will also be necessary to validate this biomarker for use in patient care.
The discovery of FOXA1 as a diagnostic marker could significantly improve the accuracy of diagnosing small cell carcinoma of the prostate, leading to better prognostic and therapeutic decisions for patients with aggressive forms of this disease.



